Many of us may from time to time, forget our neighbor’s name or the items to purchase at the grocery store, and we wonder if this is part of normal aging. Your doctor is the best person to speak with regarding these concerns. There are many conditions that are treatable that may be contributing to periodic memory lapses.
Often when we think of dementia we think of Alzheimer’s disease. While Alzheimer’s disease is considered to be the underlying cause of between 60 and 80% of all dementia cases, there are also other conditions that might cause dementia. It is important to know about the other types and causes of dementia because treatment can vary between diseases and early detection can be beneficial in slowing the progression of incurable
dementia's.
According to Dr. Harvey Gilbert, MD of the Gilbert Guide, some of the most common types of dementia and their causes are:
1. Vascular Dementia
This type of dementia is the second most common. It is caused by poor blood flow to the brain, depriving brain cells of the nutrients and oxygen they need to function normally. Vascular dementia can be caused by any number of conditions which narrow the blood vessels, including stroke, diabetes and hypertension.
2. Mixed Dementia
Sometimes dementia is caused by more than one medical condition. Most commonly, mixed dementia is caused by both Alzheimer's and vascular disease.
3. Dementia with
Lewy Bodies (
DLB)
Sometimes called
Lewy Body Disease, this type of dementia is characterized by abnormal protein deposits called
Lewy bodies that develop in nerve cells in the brain stem. This disrupts the brain’s ability to function normally and impairs cognition and behavior. It can also cause tremors and is often linked with Parkinson’s Disease and dementia. It is not reversible and there is no known cure.
4. Parkinson’s Disease Dementia (
PDD)
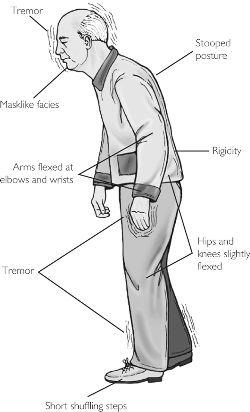
Parkinson's disease is a chronic, progressive neurological condition, and in its later stages can affect cognitive functioning. Not all people with Parkinson’s disease will develop dementia, however. This type of dementia is also a
lewy body dementia. Symptoms include tremors, muscle stiffness and speech problems. Reasoning, memory, speech, and judgment are also usually affected.
5.
Frontotemporal Dementia
Pick's disease is the most common and recognized form of
frontotemporal dementia. It is a rare disorder which causes damage to brain cells in the frontal and temporal lobes. This affects the individual’s personality significantly, usually resulting in a decline in social skills, along with emotional apathy. Unlike other
dementia's, Pick’s disease usually results in behavior and personality changes
occurring before memory loss and speech problems.
6.
Creutzfeldt-Jacob Dementia (
CJD)
A degenerative neurological disorder,
CJD is also known as “mad cow disease”. The incidence is very low, occurring in only about one in one million people. There is no cure. Caused by viruses,
CJD progresses rapidly, usually over a period of several months. Symptoms include memory loss, speech impairment, confusion, muscle stiffness and twitching, and a general lack of coordination, which makes the individual susceptible to falls. Sometimes blurred vision and hallucinations also occur with this form of dementia.
7. Normal Pressure Hydrocephalus (
NPH)
Normal pressure hydrocephalus involves an accumulation of
cerebrospinal fluid in the brain's cavities. When this fluid does not drain as it should, the associated build-up results in added pressure on the brain, interfering with the brain’s ability to function normally. Individuals with dementia caused by normal pressure hydrocephalus often experience problems with ambulation, balance and bladder control, as well as cognitive impairments involving speech, problem-solving abilities and memory.
8. Huntington’s Disease
Huntington's disease is an inherited progressive dementia that affects the individual’s cognition, behavior and movement. Symptoms include memory problems, impaired judgment, mood swings, depression and speech problems (especially slurred speech). Delusions and hallucinations may also occur. Individuals with Huntington’s disease may also experience difficulty walking, and uncontrollable jerking movements of the face and body
9.
Wernicke-
Korsakoff SyndromeWernicke-
Korsakoff syndrome is caused by a vitamin B1 (Thiamine)deficiency and often occurs in alcoholics, although it can also result from malnutrition, cancers, abnormally high thyroid hormone levels, long-term dialysis and long-term diuretic therapy (used to treat congestive heart failure). The symptoms include confusion, permanent gaps in memory, and impaired short-term memory. Hallucinations may also occur. If treated early by supplement, this dementia can be reversed.
10. Mild Cognitive Impairment (MCI)
Dementia can be due to illness, medications and a host of other treatable causes. With mild cognitive impairment, an individual will experience memory loss, and sometimes impaired judgment and speech, but they are usually aware of this decline. These problems usually don’t interfere with the normal activities of daily living. Individuals with mild cognitive impairment may also experience behavioral changes that involve depression, anxiety, aggression and emotional apathy. This is often due to the awareness of and frustration related to his or her condition.
With an understanding of the types of dementia, questions begin to arise about how these diseases are diagnosed. What can a patient expect when trying to determine whether he or she has some form of dementia? What can a caregiver expect?
When you initially meet with your doctor, it is important to be honest with them about the symptoms the patient is experiencing, their duration, frequency and rate of progression. The doctor will then review your current health status, family history and medication history. This includes evaluating the patient for depression, substance abuse and nutrition, and other conditions that can cause memory loss, including anemia, vitamin deficiency, diabetes, kidney or liver disease, thyroid disease, infections, cardiovascular and pulmonary problems. The patient also undergoes a physical exam and blood tests. Diagnosing specific diseases causing dementia can be difficult and it may be necessary to ask for a referral to a doctor with expertise in this area. Additional tests that may be used in conjunction with the aforementioned approaches include the Mini Mental State Evaluation (
MMSE), the Mini Cog Screen, and Medical Imaging (CT, MRI and PET scans).
The
MMSE is an evaluation of the patient’s cognitive status. The patient is required to identify the time, date and place where the test is taking place, be able to count backwards, identify objects previously known to him or her, be able to repeat common phrases, perform basic skills involving math, language use and comprehension, and demonstrate basic motor skills.
The Mini Cog Screen takes only a few minutes to administer, and is used as an initial screening for dementia. The patient is required to identifying three objects in the office, then draw the face of a clock in its entirety from memory, and finally, recall the three items identified earlier.
Finally, medical imaging helps doctors see images of the patient’s brain to determine whether there are any growths, abnormalities or general shrinkage which occurs in Alzheimer’s disease. These medical imaging tests can help improve the accuracy of a dementia diagnosis to 90%.
Once a diagnosis has been made, doctors can help patients to look at various treatment options and can often provide information for caregivers and families about support groups and organizations that can provide them with information about their specific diagnosis. It is recommended that patients and their families try to learn as much as they can about the disease and how it is expected to progress. Organizations like
Alzheimer’s Association or the
Parkinson's Society can provide valuable information about the disease, its progression and tips on how to slow the progression of the disease and deal with symptoms. These organizations also provide support groups to both the patient and their caregivers to help deal with the blow of a dementia diagnosis. As mentioned earlier, early detection is often key in being able to reverse or slow the progression of many of these diseases. Having a basic understanding of the many
dementia's that may occur and how they are diagnosed will be beneficial to physicians and families alike.
If you find that you simply do not know where to begin or how to handle this change in status and what it means for your future, a Geriatric Care Manager can assist you in making plans for the future.
For information on Care Managers in your area go to
http://www.caremanager.org/ or for a care manager in
Maricopa County
click here.
By
ElderCaring.ca